

A NEW PARADIGM FOCUSED ON SCIENCE, PREVENTION & SOCIAL GOOD
Every so often, a big change in thinking happens, often eliciting a so-called "paradigm shift". In our translational science setting, a paradigm is the set of concepts and standards that constitute legitimate contributions to a field – in other words, the prevailing thinking and practice that guide research, education and advocacy.
The "old" paradigm of "MIH" (molar-incisor hypomineralisation) – as introduced in 2001 and fleshed out by European paediatric dentists – revolves around a "clinical dentistry worldview" focused on the early adult teeth that emerge in 6–8 year-olds. Prevailing thoughts here centre on dental diagnosis & treatment, with standardisation not a strong point as outlined below.
The new paradigm comes from a holistic "translational worldview" that encompasses all teeth, starting with those emerging in a baby. Here, the focus is on stronger science, prevention and social good. This futuristic vision enriches the (still important) clinical dentistry perspective with viewpoints of other key stakeholders – ranging from scientists best positioned to discover cures, through medical and other branches of healthcare crucial for prevention, to supporting industry, government, and the affected public.
Our paradigm shift is triggered by three simple questions about "chalky teeth problems": (1) where do they come from?; (2) how can they be picked up early?; and (3) how might they be prevented in the first place? Such questioning then takes us to life history, as embraced by lifecourse theory, and also to the need for effective communication across all parties – from scientists through to the public.
D3G's 'MH LIFECOURSE CONCEPT' AND 'D3-CHALKY TEETH LINGO'
D3G has reconceptualised the topic of molar hypomineralisation ("MH") and chalky teeth to fit the modern ideals of science translation and preventive healthcare. Building on strengths of the DDE and MIH eras, our new 'MH lifecourse concept' embodies scientific rigour, medical prevention, and translation to social good. This revolutionary concept and its partnered language ("translational lingo") together comprise a valuable paradigm shift for the field, as acknowledged by a leading academic journal in 2024 and an industry award in 2025.
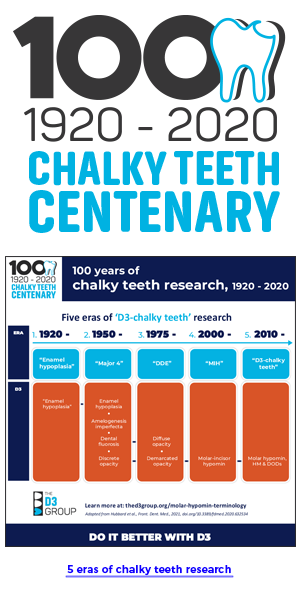
Looking back at 2010, it was clear to D3G researchers that prevailing terminology for the broader problem we today call MH was scientifically inadequate. Key limitations of the popular clinical term "molar-incisor hypomineralisation" ("MIH") were under-representation of the problem scope, and disharmony with D3G's goal of prevention. Over the following decade, D3G took a translational approach to:
(1) Develop a stronger definition for MH that emphasises scientific hallmarks and eliminates widespread confusion surrounding incisors;
(2) Introduce an underpinning classification for MH and other "demarcated opacity disorders" ("DODs") based on learnings from the scientifically-strong DDE era; and
(3) Adopt a lifecourse approach, recognising MH involves both the baby and adult teeth and so is best attacked progressively from the beginning.
(4) Craft a "translational lingo" (special language, or terminology) that enables conversation progressing from either public-friendly ("chalky teeth") or scientifically-precise starting points.
The following definition, classification and lifecourse approach to MH – which together comprise D3G's 'lifecourse concept of MH' - remain academic works in progress. This new translational concept, and its interlinked 'D3-chalky teeth lingo' (here, here), are expected to evolve both as our scientific understanding grows and the needs of diverse audiences are increasingly accommodated.
Interested parties – regardless of station, from across the sector and around the world – are encouraged to join the "D3 family" discussions that have spawned this new paradigm. You can choose to join D3G here, and/or contact us by email.
Visit here for additional information particularly pertinent to writers, reviewers and publishers.
D3G-NLM DEFINITION OF MOLAR HYPOMINERALISATION

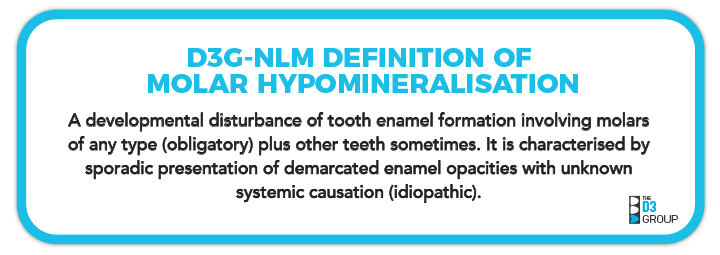
In 2023, the US National Library of Medicine (NLM, host of MEDLINE & PubMed) published a concise academic definition of Molar Hypomineralisation (MH), in association with D3G. The wording was designed to cross-reference two related bibliographic subject headings (amelogenesis, molars). NLM's dental MeSH tree was also collaboratively revised to correct misclassification of dental enamel hypoplasia and embrace clinico-scientific foundations established by Grace Suckling and contemporaries during the DDE era (D3G+NLM, manuscript in preparation). D3G added translational value to NLM's definition by emphasising both sporadic presentation and unknown systemic causation (idiopathic) as scientific hallmarks of MH, and describing the enamel-formation process more simply.
Our ensuing concise academic definition of MH is:
This field-reshaping advance followed widespread consultation and peer review, both across the sector and around the world (Toronto International D3 Symposia, 2020-2022), together with publication of a historical review of "chalky teeth research". This consensus-seeking process also prompted development of an MH Green Paper, that supports not only the above concise academic definition, but also provides three other definitions of MH optimised for specialist, professional and public audiences (see below).
DRAFT CLASSIFICATION OF MH AS A 'DEMARCATED OPACITY DISORDER'
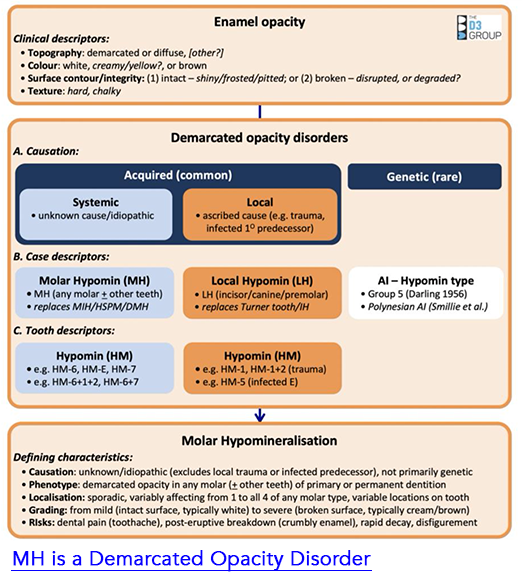
Surprisingly, a published classification was lacking for MH, perhaps reflecting the common misconception it is a (relatively) "new condition". To provide clinical and scientific context for our definition of MH, D3G has drafted a classification scheme for MH and other conditions involving dental enamel opacities that appear solidly distinct from normal enamel (i.e. "demarcated", as opposed to "diffuse") – we collectively term these "demarcated opacity disorders" or "DODs" for short.
Having gone largely unrecognised until late in the first century of chalky enamel research, MH needs to be considered in view of what came earlier, particularly during the DDE era. Such clinical and scientific appraisals indicate MH is a distinct type of DOD. Classification of MH therefore necessitates formulation of a broader scheme embracing other known DODs and enamel opacities in general. As portrayed in our draft DOD Classification infographic (right, published here), once demarcated opacities are defined as a subgroup of enamel opacities, attention turns to their primary causation (acquired or genetic). Acquired DODs are then categorised at case level as having systemic origins (e.g. MH), as distinct from local causation. MH cases can then be characterised at hypomineralised (HM) tooth level by combining two popular dental notations to distinguish baby and adult dentitions.
Beneficially in both the clinic and lab, this strategy provides a translationally-robust, diagnostic flow from demarcated opacity to "HM tooth" to "MH kid". Further details appear in our MH Green Paper (see below).
A LIFECOURSE APPROACH TO MH
By embracing the whole dentition – from earliest baby teeth through to wisdom teeth in early adulthood – D3G's scientific approach to "MH" enjoys all the medical and social benefits of modern lifecourse theory. This "timeline approach" follows an individual's life history from the beginning and considers multiple influences (e.g. medical, environmental, socioeconomic) during development from a baby into adulthood. Strong alignments can then be made with the medical origins of MH, maternal and child health and allied inequality issues. Importantly, this lifecourse platform also highlights MH as a potentially preventable birth defect – as explained to families in 'Sam's Story'.
Our switch to 'MH lifecourse' thinking has necessitated a major revision of terminology and clinical reporting. Hence, we refer to back teeth at most risk of being chalky in order of their eruption into the mouth – starting with 2-year molars, then 6-year and 12-year molars, and finally the wisdom teeth (18-year molars). Our unique compilation of MH prevalence studies exemplifies this new approach, and ensuing benefits for MH prevention at dental and medical levels are noted below.
ACADEMIC CASE & LEAD ADOPTERS OF THE NEW PARADIGM
D3G's academic case for evolving D3 terminology and introducing our lifecourse concept of MH involved three
main initiatives:
(1) Resolving chaos of the MIH era (see below);
(2) Better referencing of the scientifically-strong DDE era; and
(3) Establishing a lifecourse platform for MH.
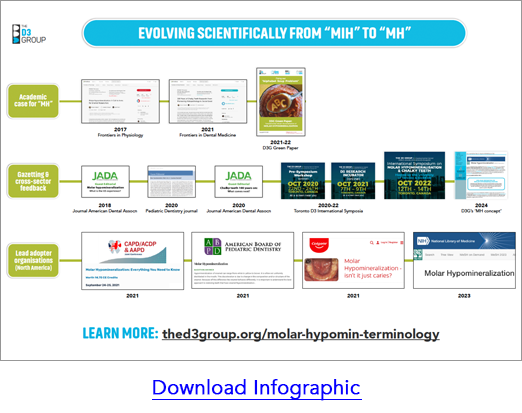
Publicising this work commenced with the 2017 publication of
a call to arms article about MH that targetted scientifically-inclined readers. Such emphasis on a cohesive whole-dentition mindset was shared with clinical audiences via
guest editorials in widely-read dental journals (JADA 2018, Pediatric Dentistry 2020, JADA 2020). Translational exposure
to interested parties from across the sector and around the world was achieved via our Toronto D3 Symposia (2020, 2021, 2022) and accompanying MH Green Paper (see below). During this time, North American paediatric dentistry organisations (AAPD, CAPD, ABPD), and an educationally-active multinational company (Colgate), embraced the term "MH" independently in far-reaching educational settings, as illustrated in this infographic. The term "MH" also starred in a top-ranking scientific journal (Proceedings of the National Academy of Science, USA) in 2022. Adding wonderful icing to this D3 cake, USA's authoritative National Library of Medicine (NLM) did a long-needed "D3 makeover" at bibliographic-database level, including the concise academic definition of MH above. This was followed in 2024 with the first adoption by an academic journal of D3G's translational paradigm (Pediatric Dentistry editorial), marking a major milestone for the MH Lifecourse concept. In 2025, D3G received an industry award recognising the above contributions to worldwide oral health.
WHAT BENEFITS DOES "MH" HAVE OVER "MIH ALPHABET SOUP"?
As elaborated here, the MIH era benefitted our field by increasing awareness around MH, particularly in clinical dentistry and worldwide prevalence contexts. Unfortunately, those two "MIH decades" became plagued by terminological chaos – which we nickname "the alphabet soup problem" (see below). In contrast to this fragmented era of "MIH alphabet soup", the holistic thinking behind our D3G-NLM definition of MH has three core benefits, each aligning with D3G's science to social good mission.
1. STRONGER SCIENCE
![]()
Full scope of the problem:
As a case descriptor, "MH" addresses the whole problem of idiopathic demarcated opacities, as they present across both dentitions (i.e. baby and adult teeth). Conversely, "MIH" involves early-erupting adult teeth only, and so risks "tunnel vision" – both scientifically and clinically. Consequent reliance on other terms for baby and later-erupting adult teeth also gives false impression of distinct conditions (e.g. MIH, HSPM, HOPT; see below) – rather than the reality of MH being a medico-dental "spectrum disorder".
Understanding causation:
Critically for investigation of medical causation (aetiology), "MH" avoids the diagnostic uncertainties associated with chalky adult incisors. In contrast, "MIH" is aetiologically compromised by uncertainties whether demarcated opacities on adult incisors have local origins (so-called "Turner teeth") or systemic origins – technically, this uncertainty is called aetiological confounding. Focussing instead on molars at case level provides an "aetiologically clean" way to study the medical origins (i.e. idiopathic, systemic causation) and prevention of MH. What then happens to hypomineralised adult incisors, which remain problematic for clinicians and affected kids alike? Generally, it's best to "drop" from case- to tooth level and simply call them "hypomin incisors" (HM-incisors) – this avoids the causation issue. However, when HM-incisors seemingly do have idiopathic systemic causation, then they (and any other teeth with idiopathic demarcated opacities) are scientifically included in an "MH" case (read more).
2. BETTER PREVENTIVE PRACTICE
'MH lifecourse' approach:
As above, by including all teeth in the baby and adult dentitions, D3G's 'MH lifecourse' approach aligns with the medical, environmental and socioeconomic considerations of modern lifecourse theory. The holistic nature of ensuing understanding (the "gestalt of MH") will benefit both clinical and public-health practice. From a prevention standpoint, this approach provides a logical order of attack and makes for easy communication about the invisible delay between a child's age at medical onset of chalky enamel (i.e. when hypomineralisation happened inside the jaw) and later "dental ages" when chalky teeth erupt into the mouth (2-year, 6-year, 12-year & 18-year molars) – see D3G's tooth eruption chart. Conversely, "MIH" addresses just the middle part of this dental spectrum (6-year molars), leading to the "alphabet soup" of terms describing other stages and manifestions.
Dental prevention:
Targetting preventive healthcare at population level, D3G's 'MH lifecourse' approach encourages "chalky teeth screening" from early ages (e.g. 18+ months for chalky baby canines, 24+ months for chalky 2-year molars) – see pilot studies in New Zealand and Canada. Such early detection maximises not only opportunities for dental professionals to act preventively, but also enables affected families and their dental advisors to anticipate chalky teeth erupting at later ages. As a result of this preventive strategy, identified "chalky teeth kids" may have substantially lower need for complicated (expensive) dentistry. Conversely, "MIH" is unhelpful in this regard, being focussed on adult teeth only.
Medical prevention:
If we're to learn how to prevent MH medically – that is, by stopping chalky enamel (hypomineralisation) from happening in the first place – we must understand its causation across the full range of medical-onset ages. The medical origin of MH spans from birth (baby teeth) through to adolescence (wisdom teeth). Our "MH lifecourse" approach supports this quest, whereas "MIH" again risks "tunnel vision" aetiologically.
3. SOCIAL GOOD
'D3 science to social good':
Together, MH affecting 1 in 5 kids worldwide, plus its associated burden of tooth decay, dental pain and psychosocial issues,, underpins massive social damage across our planet. A correspondingly huge opportunity to benefit global society seems likely once a medical-prevention strategy is identified and successfully implemented. To achieve this exciting goal, we need strong science and an 'MH lifecourse' approach as noted above. From first principles at least, we can surely expect that "translational MH thinking" will get us there much faster than "MIH tunnel vision" and all its chaotic baggage.
'Good for D3 science':
A reciprocal benefit of stronger D3 science being good for society is that social awareness of the chalky teeth/MH problem should benefit scientific endeavours to prevent it.
"ALPHABET-SOUP PROBLEM" AND OUR "MH GREEN PAPER" SOLUTION
Urgent need for a translationally robust characterisation of MH became a catch-cry of the 2020 D3 Workshop – our inaugural international-consensus-seeking event for "Molar Hypomin and Chalky Teeth". Particular concerns revolved around the chaotic – and scientifically untenable – set of terms that had been published over the preceeding 20 years (i.e. MIH era). Drawing on the alphabet soup metaphor, we nicknamed this "the Alphabet Soup Problem".
The MIH era's "Alphabet Soup Problem"
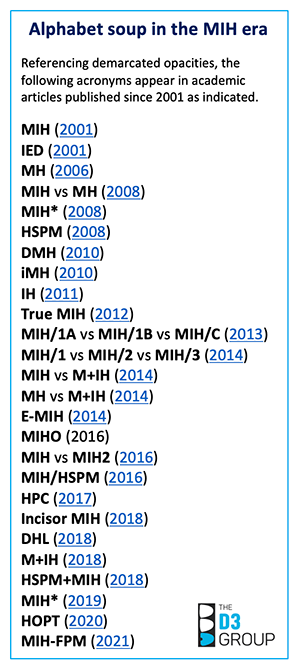
Scientifically at least, it's disturbing that the academic literature has accumulated at least 25 other terms referencing “demarcated opacities” since the term “MIH” (molar-incisor hypomineralisation) was introduced in 2001. The most-prevalent accessory terms include "HSPM", "DMH" and "IH" – standing for hypomineralised second primary molars (same thing as 2-year molars), deciduous molar hypomineralisation and incisor hypomineralisation, respectively. Yet key gaps remain despite this confusing "MIH alphabet soup". A notable absence is hypomineralised 12-year molars which comprise a second type of "HSPM" (hypomineralised second permanent molars) by above convention – talk about confusing! The same goes with "HPC" representing hypomineralised primary canines only (not the permanent canine type of HPC). Is this shemozzle of terms and acronyms good for science, clinical practice and communication? Clearly not – but what to do about it and how?
D3G's Green Paper on "Fixing our Alphabet Soup Problem"
Unsurprisingly given our translational mission, D3G invited all main stakeholders (scientists & researchers, dental & medical practitioners, educators, publishers, industry, research funders, government and affected public) to team up and fix this "alphabet soup problem” together. Drawing on a decade of listening, learning and testing the waters, the "D3G brain trust" drafted a Green Paper outlining translational characterisation of MH that's both scientifically robust and historically accurate. This first draft – which focussed on classification, audience-specific definitions, terminology, grading, and clinical recording of MH – was shared as "pre-event homework" at the 2021 D3 Research Incubator (video highlights). Over 110 participants representing 30 countries and all major stakeholder groups were exposed to the document.
The second draft was subjected to a further two refinement steps in 2022 – firstly at a Pre-symposium Task Force meeting on Clinico-scientific Standards (14 experts from 8 countries), then subsequently at the 2022 D3 Symposium in Toronto where a broader translational perspective was available (100+ participants from 22 countries). Altogether, over 50 people are acknowledged for their contributions, including DDE wonder woman Grace Suckling, and three pioneers of the MIH era (Birgitta Jalevik, Anna Maria Vierrou, Marlies Elfrink). With a working consensus achieved at "D3 aficionado" level, D3G is now striving to ensure broader workability of our "MH-Demarcated Opacity Disorder concept" across the sector and around the globe. For starters, the latest iteration was provided to a broad research-centric audience (researchers, educators, practitioners, publishers) attending our D3 Day at IADR-2024, and selected content continues to be publicised at various D3G events since then and on this website (including reporting guidelines here).
Interested individuals can access the 'MH Green Paper' – volubly titled "Fixing our Alphabet Soup Problem. D3G Green Paper on translationally robust characterisation of Molar
Hypomineralisation and other demarcated opacity disorders"
– through our D3 Learning Loop.
HELPING WRITERS & REVIEWERS "MAKE THE SWITCH TO D3"
Visit D3 Reporting to learn more about the evolution of this new translational paradigm as a cross-sector initiative, allied goals for standardised D3 reporting, and "How To" guides for those upgrading from "MIH" to "D3" world views.
LEARN MORE AND SHARE YOUR THOUGHTS
Learn more about how we've integrated the MH Lifecourse Concept across key stakeholder groups, particularly FAMILIES (What is Molar Hypomin?), COMMUNITY (Prevalence) PRACTITIONERS (D3 Terminology), and RESEARCHERS (D3 Reporting).
As always at D3G, your feedback and enquiries are welcomed (contact us).